The Relationship between Blood Pressure Response Index and Acute Kidney Injury in Patients with Septic Shock: A Retrospective Study Based on the MIMIC-IV Database
DOI:
https://doi.org/10.71321/61pvj246Keywords:
septic shock, acute kidney injury, blood pressure response index, intensive care unit, MIMIC-IV databaseAbstract
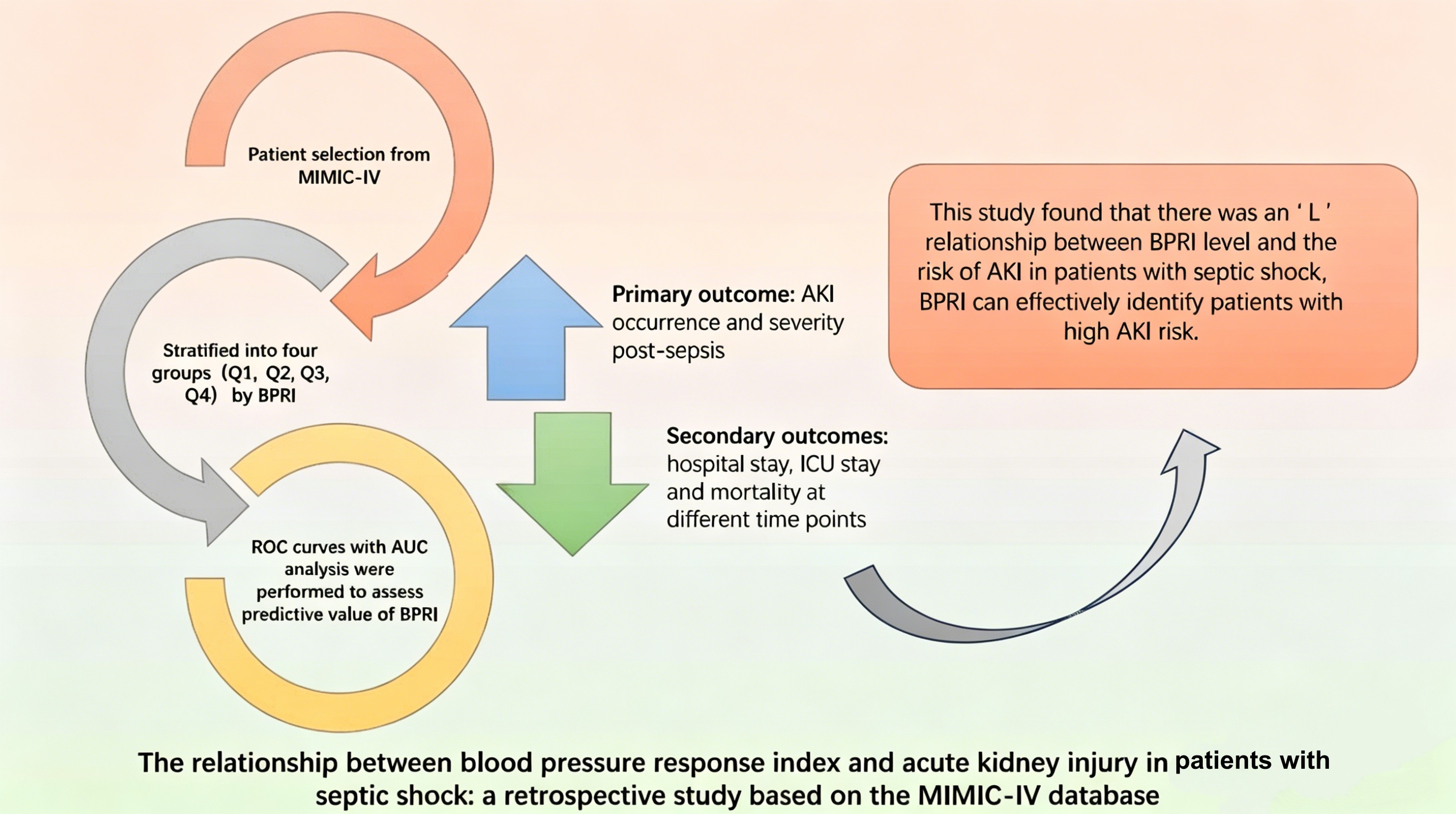
Background: The blood pressure response index (BPRI) is the ratio of mean arterial pressure (MAP) to the vasoactive-inotropic score (VIS). It accurately reflects the response to vasoactive drugs in patients with septic shock and assesses the patient's vascular status. However, the relationship between BPRI and the occurrence of acute kidney injury (AKI) in patients with septic shock has never been studied.
Methods: This study retrospectively analyzed patients diagnosed with sepsis and using vasoactive drugs in the MIMIC-IV database. The patients were divided into four groups according to the BPRI level. The primary outcome is whether AKI occurs after the diagnosis of sepsis. The association between BPRI and outcome was assessed by constructing logistic regression models and plotting restricted cubic spline (RCS) curves. The predictive value of the BPRI for outcome was evaluated by plotting receiver operating characteristic (ROC) curves and comparing areas under the curves (AUC).
Results: 5524 patients with septic shock were finally included. The median age of the patients was 68.8 years, and 84.3% developed AKI after the diagnosis of sepsis. In a fully adjusted model, BPRI and the development of AKI were significantly correlated (OR [95%CI], 0.988 [0.979, 0.996], P=0.006). The results of the RCS curves suggested an "L"-shaped association and the inflection point was located at the level of 3.98. On the left side of the inflection point, there was a decreasing trend in the risk of AKI in patients as BPRI levels increased (OR [95%CI], 0.82 [0.747, 0.9], P<0.001). On the right side of the inflection point, there was no statistically significant association (OR [95%CI], 0.995 [0.985, 1.01], P=0.212). In addition, the BPRI showed favorable predictive value for outcome (AUC [95% CI], 0.624 [0.601, 0.639]).
Conclusion: We identified a distinct non-linear association between BPRI and AKI risk in septic shock, characterized by a critical inflection point at 3.98. Below this threshold, the likelihood of AKI rises sharply as BPRI decreases. Integrating perfusion pressure and vasopressor load, the BPRI serves as a readily available metric to stratify renal risk and recognize vascular hyporesponsiveness.
References
[1] Zampieri FG, Bagshaw SM, & Semler MW. (2023). Fluid Therapy for Critically Ill Adults With Sepsis: A Review. Jama, 329(22), 1967–1980. https://doi.org/10.1001/jama.2023.7560
[2] Oppert M, Engel C, Brunkhorst FM, Bogatsch H, Reinhart K, Frei U, et al. (2008). Acute renal failure in patients with severe sepsis and septic shock--a significant independent risk factor for mortality: results from the German Prevalence Study. Nephrol Dial Transplant, 23(3), 904–909. https://doi.org/10.1093/ndt/gfm610
[3] Zarbock A, Nadim MK, Pickkers P, Gomez H, Bell S, Joannidis M, et al. (2023). Sepsis-associated acute kidney injury: consensus report of the 28th Acute Disease Quality Initiative workgroup. Nat Rev Nephrol, 19(6), 401–417. https://doi.org/10.1038/s41581-023-00683-3
[4] Peerapornratana S, Manrique-Caballero CL, Gómez H, & Kellum JA. (2019). Acute kidney injury from sepsis: current concepts, epidemiology, pathophysiology, prevention and treatment. Kidney Int, 96(5), 1083–1099. https://doi.org/10.1016/j.kint.2019.05.026
[5] Evans L, Rhodes A, Alhazzani W, Antonelli M, Coopersmith CM, French C, et al. (2021). Surviving sepsis campaign: international guidelines for management of sepsis and septic shock 2021. Intensive Care Med, 47(11), 1181–1247. https://doi.org/10.1007/s00134-021-06506-y
[6] Font MD, Thyagarajan B, & Khanna AK. (2020). Sepsis and Septic Shock - Basics of diagnosis, pathophysiology and clinical decision making. Med Clin North Am, 104(4), 573–585. https://doi.org/10.1016/j.mcna.2020.02.011
[7] Monnet X, Lai C, & Teboul JL. (2023). How I personalize fluid therapy in septic shock? Crit Care, 27(1), 123. https://doi.org/10.1186/s13054-023-04363-3
[8] Mok G, Hendin A, Reardon P, Hickey M, Gray S, & Yadav K. (2021). Macrocirculatory and Microcirculatory Endpoints in Sepsis Resuscitation. J Intensive Care Med, 36(12), 1385–1391. https://doi.org/10.1177/0885066620982585
[9] Frenkel A, Abuhasira R, Fisher L, Bichovsky Y, Zlotnik A, Novack V, et al. (2023). Vasopressors and Mean Arterial Pressure in Septic Shock: Do We Bend the Rules for Young Adults? Isr Med Assoc J, 25(11), 741–746.
[10] Belletti A, Lerose CC, Zangrillo A, & Landoni G. (2021). Vasoactive-Inotropic Score: Evolution, Clinical Utility, and Pitfalls. J Cardiothorac Vasc Anesth, 35(10), 3067–3077. https://doi.org/10.1053/j.jvca.2020.09.117
[11] Chen Y, Jiang H, Wei Y, Qiu Y, Su L, Chen J, et al. (2024). Blood pressure response index and clinical outcomes in patients with septic shock: a multicenter cohort study. EBioMedicine, 106, 105257. https://doi.org/10.1016/j.ebiom.2024.105257
[12] Johnson AEW, Bulgarelli L, Shen L, Gayles A, Shammout A, Horng S, et al. (2023). MIMIC-IV, a freely accessible electronic health record dataset. Sci Data, 10(1), 1. https://doi.org/10.1038/s41597-022-01899-x
[13] Singer M, Deutschman CS, Seymour CW, Shankar-Hari M, Annane D, Bauer M, et al. (2016). The Third International Consensus Definitions for Sepsis and Septic Shock (Sepsis-3). Jama, 315(8), 801–810. https://doi.org/10.1001/jama.2016.0287
[14] Han J, Pinsino A, Sanchez J, Takayama H, Garan AR, Topkara VK, et al. (2019). Prognostic value of vasoactive-inotropic score following continuous flow left ventricular assist device implantation. J Heart Lung Transplant, 38(9), 930–938. https://doi.org/10.1016/j.healun.2019.05.007
[15] KDIGO 2021 Clinical Practice Guideline for the Management of Glomerular Diseases. (2021). Kidney Int, 100(4s), S1–s276. https://doi.org/10.1016/j.kint.2021.05.021
[16] Eckardt KU, Bernhardt WM, Weidemann A, Warnecke C, Rosenberger C, Wiesener MS, et al. (2005). Role of hypoxia in the pathogenesis of renal disease. Kidney Int Suppl, 10.1111/j.1523-1755.2005.09909.x(99), S46–51. https://doi.org/10.1111/j.1523-1755.2005.09909.x
[17] Nath KA, & Norby SM. (2000). Reactive oxygen species and acute renal failure. Am J Med, 109(8), 665–678. https://doi.org/10.1016/s0002-9343(00)00612-4
[18] Liu J, Xie H, Ye Z, Li F, & Wang L. (2020). Rates, predictors, and mortality of sepsis-associated acute kidney injury: a systematic review and meta-analysis. BMC Nephrol, 21(1), 318. https://doi.org/10.1186/s12882-020-01974-8
[19] White KC, Serpa-Neto A, Hurford R, Clement P, Laupland KB, See E, et al. (2023). Sepsis-associated acute kidney injury in the intensive care unit: incidence, patient characteristics, timing, trajectory, treatment, and associated outcomes. A multicenter, observational study. Intensive Care Med, 49(9), 1079–1089. https://doi.org/10.1007/s00134-023-07138-0
[20] Badin J, Boulain T, Ehrmann S, Skarzynski M, Bretagnol A, Buret J, et al. (2011). Relation between mean arterial pressure and renal function in the early phase of shock: a prospective, explorative cohort study. Crit Care, 15(3), R135. https://doi.org/10.1186/cc10253
[21] Wang M, Wang X, Zhu B, Li W, Jiang Q, Zuo Y, et al. (2023). The effects of timing onset and progression of AKI on the clinical outcomes in AKI patients with sepsis: a prospective multicenter cohort study. Ren Fail, 45(1), 1–10. https://doi.org/10.1080/0886022x.2022.2138433
[22] Annane D, Ouanes-Besbes L, de Backer D, Du B, Gordon AC, Hernández G, et al. (2018). A global perspective on vasoactive agents in shock. Intensive Care Med, 44(6), 833–846. https://doi.org/10.1007/s00134-018-5242-5
[23] Priyanka P, Chang CH, Chawla LS, Kellum JA, Clermont G, & Murugan R. (2022). VASOPRESSOR-RESISTANT HYPOTENSION, COMBINATION VASOPRESSOR THERAPY, AND SHOCK PHENOTYPES IN CRITICALLY ILL ADULTS WITH VASODILATORY SHOCK. Shock, 58(4), 260–268. https://doi.org/10.1097/shk.0000000000001980
[24] Hou K, Chen Q, Zhu X, Shen X, Zou L, Mu X, et al. (2021). Correlation Between Vasoactive-Inotropic Score and Postoperative Acute Kidney Injury after Cardiovascular Surgery. Heart Surg Forum, 24(2), E282–e292. https://doi.org/10.1532/hsf.3537
[25] Hoste EA, Damen J, Vanholder RC, Lameire NH, Delanghe JR, Van den Hauwe K, et al. (2005). Assessment of renal function in recently admitted critically ill patients with normal serum creatinine. Nephrol Dial Transplant, 20(4), 747–753. https://doi.org/10.1093/ndt/gfh707
[26] Makris K, & Spanou L. (2016). Acute Kidney Injury: Diagnostic Approaches and Controversies. Clin Biochem Rev, 37(4), 153–175.
[27] Prowle JR, Echeverri JE, Ligabo EV, Ronco C, & Bellomo RJNRN. (2010). Fluid balance and acute kidney injury. 6(2), 107–115.
[28] Harrois A, Grillot N, Figueiredo S, & Duranteau J. (2018). Acute kidney injury is associated with a decrease in cortical renal perfusion during septic shock. Crit Care, 22(1), 161. https://doi.org/10.1186/s13054-018-2067-0
[29] Le Dorze M, Bouglé A, Deruddre S, & Duranteau JJS. (2012). Renal Doppler ultrasound: a new tool to assess renal perfusion in critical illness. 37(4), 360–365.
[30] Malik J, Lomonte C, Meola M, de Bont C, Shahverdyan R, Rotmans JI, et al. (2021). The role of Doppler ultrasonography in vascular access surveillance-controversies continue. J Vasc Access, 22(1_suppl), 63–70. https://doi.org/10.1177/1129729820928174
[31] Koratala A, & Reisinger N. (2022). Venous Excess Doppler Ultrasound for the Nephrologist: Pearls and Pitfalls. Kidney Med, 4(7), 100482. https://doi.org/10.1016/j.xkme.2022.100482
Type
Published
Data Availability Statement
The datasets generated and analyzed during this study can be accessed from the MIMIC-IV database at https://mimic.physionet.org/iv/, or obtained from the corresponding author upon reasonable request.
Issue
Section
License
Copyright (c) 2026 Life Conflux

This work is licensed under a Creative Commons Attribution 4.0 International License.
How to Cite





